Richard Tice and Reform’s money - the new unanswered question: ‘This is a question that cuts to the core of who funds British politics - and who funds Reform.’
Recently I read:
It’s the end of Reform as we know it: We can but hope, unless it gets replaced by something even worse.
Anthropic’s AI Claude hacked into three organizations during cybersecurity test
Latest posts:
Providing the greatest educational resources to people who do well on tests isn't the only option
I’m sure Yglesias' post in response to the recent SCOTUS ruling against affirmative action will generate plenty of heated debate. But I was struck by one of the points that’s not really about affirmative action at all, or at least not along the dimensions of identity we mostly commonly think about with this topic.
Part of the benefits of being allowed into an elite US university is that they’re tremendously well resourced. Harvard’s endowment fund was worth an astonishing $53 billion recently. It could provide a huge amount of the best quality educational resources to it’s ~21k students.
But should it?
“…the smarter you are at age 18, the more educational resources you should receive” is not an obviously correct allocation of social resources.
It may be an empirical matter as to what educational distribution model is best for a given society. But first we’d have to define what “best” even means. I’m sure there are many highly conflicting opinions out there on that.
Perhaps today’s division of educational resources is the ideal arrangement for some outcome. But it’s certainly not some kind of natural law that the lion’s share of these resources must go towards the people who already did particularly well on a test when they were a child.
Especially insomuch as the sort of people who do well on school tests and, even moreso, gain access to elite institutions today tend to be those who already had access to the most resources since the day that they were born.
Absolutely obsessed with The Password Game.
All the fun of trying to pick a computer password suitable for one’s corporate accounts, but with…even more fun than this screenshot lets on. Doubt I’ll ever come close to “winning” though.

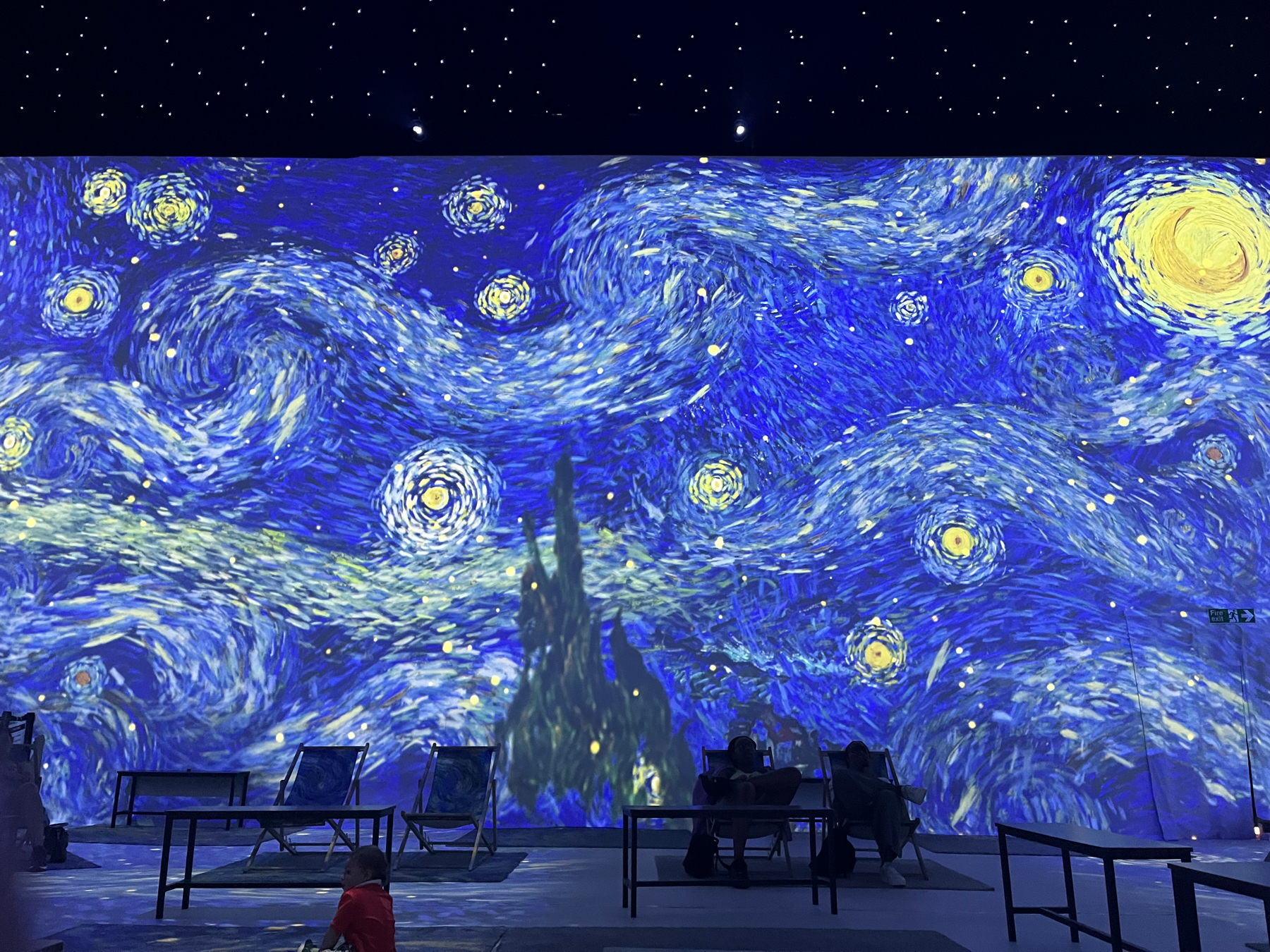
A trip to the Van Gogh Immersive Experience
A couple of weeks ago I went to the Van Gogh Immersive Experience in London.
Here’s the gentleman in question.

Although I’m in general artistically ignorant, I was already a fan particularly of his extremely famous “Starry Night”. The exhibition was kind of short and a bit gimmicky in places, but I do feel like I came away with a deeper appreciation and knowledge of the fellow and a deeper awareness of his art so I’m overall happy enough to have gone.
One such new-to-me fact was that Van Gogh was thought to be colourblind. This may be what is behind his iconic use of colour. Perhaps he literally saw the world differently to most of us do.
Born in 1853, Van Gogh was an even more tortured soul than I had realised. Famously he had psychotic episodes, worsening over his life. These occurred alongside bouts of depression, epilepsy and possibly bipolar disorder. Without the necessary support it could make him hard to live with at times; the well-known cutting his own ear off incident apparently occurred shortly after a huge row with a housemate.

He was fully aware of his condition and the concomitant delusions, checking himself into a psychiatric hospital after the ear event. Even inside such a place he was artistically productive when not entirely incapacitated, producing some of his very widely known pieces of art. Sometimes these were based only on what he could see out of his room’s window, other times by the contents of his dreams: “I dream of painting and then I paint my dream”. Over his lifetime he produced over 2000 artworks.
Eventually he was deemed fit and safe to go return to the outside world. Unfortunately it was too soon. On the last day of his life, July 27th 1890, aged 37, he painted one final picture, Tree Roots, and then, a couple of hours later, shot himself in the chest. It wasn’t an instantaneous death, but two days later he was no longer with us.
Sadly, Van Gogh wasn’t at all well-known or renowned during his life. The excitement around (and incredible valuations of - some have since sold for the equivalent of hundreds of millions of dollars) his paintings came much later.
The main titular “immersive” part of the exhibition occurs at the end of the show where you get to sit in a deck chair in a big dark room surrounded by animations based on his most famous paintings and quotes, with an appropriate soundtrack for as long as you feel like witnessing the loop.

Pragmatically, it must be said that given the surfeit of excellent and free museums and galleries in London this one is pretty expensive for what it is. That said, I guess the immersive part of it probably isn’t available anywhere else so if you want to see that there’s little choice.
My pro tip if you have some-but-not-infinite cash to burn would be to buy the standard ticket (£18 per adult), not the VIP one (£27.90), even if you want to have a go at the extra VR experience. You can buy entrance to the VR part when you’re there if you want, currently for £5. VIPs can queue-skip, but then again I went on a random Sunday and there was no queue at all. You also don’t get a poster to go home with, but there’s plenty to be had in the gift shop.
Mya Gosling provides what turns out to be a handy guide to the 7 Shakespeare plays that might accidentally be banned in parts of the US should their ridiculous anti-drag show legislation actually become law.

Good Tickle Brain contains a huge supply of Shakespearean webcomics should you need more.
Huge shock to the system today when I saw what appeared from a distance to be a dead human body on the roadside.

Fortunately upon closer inspection it turned out to be simply something I might characterise as village weirdness. Still rather needs an explanation though.
Living in the dumbest timeline as we do, the president of the Ultimate Fighting Championship has apparently confirmed that the Zuckerberg vs Musk cage match, and event that sounded so The Onion it didn’t even register as potentially real in my mind, is “absolutely dead serious”.
I mean it probably won’t happen, given that a good proportion of what Elon says these days doesn’t happen. But I also wouldn’t entirely rule it out, especially if there’s a possibility for the $100 pay-per-view show that UFC President White indicates there is.
Keenan has it right with their swear-word ridden headline.
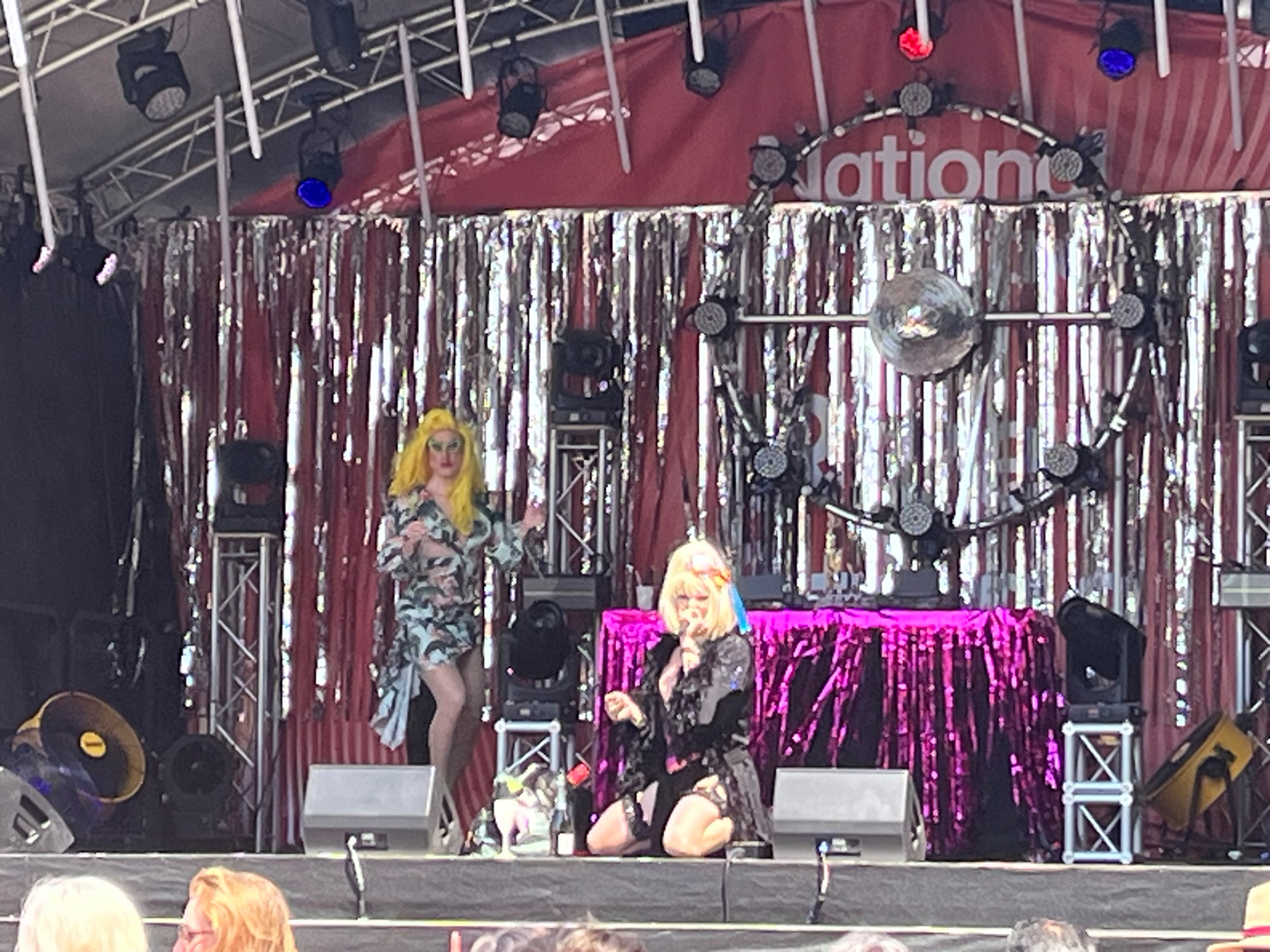
A day of musical fun in the sun, perhaps to be banned in the US
It’s been a couple of weeks since I had a wonderful day out in London with a well-connected friend, enjoying activities that might soon be illegal in parts of the US.
We braved the heat, fueled only by frozen variations of cocktails, to take advantage of the many free festivals that were on offer that weekend.
First up we saw the self-proclaimed “first Black Drag King from Birmingham to have been featured on Channel 4”: the incredible Don One.

This was on the riverside pedestrian area somewhere outside of the South Bank Centre if I recall correctly, so there was no roof to raise but without question it would have been had there been one.
They’ve a Youtube channel for anyone interested in experiencing the Don1 vibe.
Next up, I’m afraid I didn’t catch the name of this duo, but they were a couple of hilarious drag queens with maximum lip syncing and audience interaction. They took a small break in the middle so they could have a quick on-stage prosecco brunch, entirely understandable given the sunshine.
Then a few streets away from, and unrelated to, the drag stage, I got to witness The Yes Mess, whom you can also take a look at on their Youtube channel.
Although that vid that doesn’t feature one of my favourite parts of that weekend’s show; the live oboe performances.

Why my “illegal in the US” comment above? Well, it relates to the drag performances that formed part of the above adventures.
As part of the Republican effort to invalidate any minority that doesn’t look and behave exactly like Donald Trump, some of their politicians and lawmakers are attempting to introduce bans on drag shows.
This isn’t hyperbole. I’d foolishly assumed that “drag ban” was a catchy name in general for the ever more horrific legislation around gender and sexuality certain US states are producing rather than something literally relating to drag shows. And although it’s undoubtedly a part of the same effort, there are restrictions or bans specifically for drag shows being proposed.
From the Guardian:
Most of the proposed bills include defining a drag performer as someone performing while using dress, makeup and mannerisms associated with a gender other than the one assigned to them at birth.
It’s an absolutely ridiculously restriction on the supposedly sacred freedom of expression value the same folk likely claim to hold dear. The thought that some of the folk enriching our lives by providing hilarious and harmless weekend entertainment could be prosecuted for doing so is truly mind-blowing.
Not that this style of performance would necessarily be what the impact would be limited to. As is typical, laws designed to cause anguish to a section of society that the proposers don’t credit as having any moral worth to worry about whatsoever tend to spill over to other areas. Famously, the definition above would presumably ban the several of Shakespeare’s plays that have storylines involving cross-dressing. This is especially ironic given that back in the day all of their female characters would have been played by men.
I’m really not convinced that watching Mrs Doubtfire - presumably first in line to lose its PG rating - when I was a kid did me permanent harm. Although having not watched it in a while I also don’t know if it aged well.
Intrigued to learn that the RStudio folks are actively working on an integration with the GitHub Copilot generative AI coding assistant.
As I spend so much time inside RStudio I haven’t yet bothered to give Copilot a go despite the rave reviews. I’m sure this will induce me to do so.
US residents can join class actions against Google and Facebook's abuse of their data
Anyone in the US who did a Google search between 2006-2013 might like to sign up here before the end of July 2023 in order to join a class action lawsuit against them.
Google has committed to pay out $23 million dollars in total, although given rather a lot of people did use Google over that 7 year period it’s thought to be likely to come out at about $7 per claimant. So honestly it’s this is just a very minor cost of doing business for Google unfortunately.
Why the payout? Surprise surprise, it’s ad-driven big tech misusing your personal data once again.
From the NYT’s report:
The consolidated class-action lawsuit filed in 2013 accused the company of “storing and intentionally, systematically and repeatedly divulging” users' search queries and histories to third-party websites and companies.
This is seen as a violation of privacy laws as well as defying what Google itself claimed to be doing to its users. It’s a particular issue because people often search for something quite personal to themselves. We’ve largely been trained to feel unconstrained in our searching - Google is the first port of call for many who suspect they are suffering from a medical issue for instance - despite the fact that in reality these days you might often assume that anything you type into the internet will one day be divulged to someone you didn’t expect to see it.
Google search queries often contained sensitive and “personally identifiable” information, including “users' real names, street addresses, phone numbers, credit card numbers, Social Security numbers, financial account numbers and more, all of which increases the risk of identity theft
Facebook is also in similar trouble for its unconstrained sharing of your personal data to various external groups, including the infamous Cambridge Analytica.
Facebook’s parent company, Meta, agreed last year to settle a class-action lawsuit that accused the company of sharing user data or making it accessible to third parties, including the data and political consulting firm Cambridge Analytica, without users’ permission
If you used Facebook between May 2007 and December 2022 in the US then sign up here before August 25th 2023 to apply for your share of a $725 million payout.
I think both these actions require you to have been a US resident during the relevant period, although I can’t say I’ve looked into what exactly the technical definition of that is.
Jenara Nerenberg asks us to consider a different type of diversity in "Divergent Mind"
📚 Finished reading: Divergent Mind by Jenara Nerenberg.

This book encourages us to consider a type of diversity less commonly considered in mainstream diversity, equity and inclusion efforts: the differences in how people think and feel, with a focus on how they process sensory input.
“Temperament rights” captures the idea that we should respect individual’s temperament and neurology in the same way that we should respect other aspects of people such as their gender, sexuality, or ethnic identity.
Much of the focus is on people with high sensitivity. This is commonly an aspect of diagnoses like autism, ADHD, sensory processing disorder, synesthesia or those termed “highly sensitive people”, as well as present in plenty of people who have no medical diagnosis at all.
Living in a world not attuned for ones' sensory processing can be overwhelming, exhausting and frustrating. Things that seem perfectly normal to other people - loud music, crowds - can be very stressful. “Everyday” tasks we’re all supposed to be able to do such as housework or adhering to deadlines might be difficult. At the same time they might truly excel in other areas of life.
The difficulties are compounded by the pressure those with these conditions feel to fit in, to appear “normal” throughout life. They do this by masking their experience. They may feel compelled to do this in every aspect of life, including in social and workplace environments, silently facing an extra challenge many of us do not. Women are apparently particularly prone to this, with their behaviour in general being more policed within our patriarchal society, having been socialised to mask more often and more effectively.
Of course this comes at a cost. Sufferers may appear to lash out or exhibit other behaviours determined by many to be “bad”. They commonly present with comorbidities such as depression anxiety, shame, guilt, low self-esteem, suicidal thoughts and distorted self-image. Masking by definition precludes you from living a life in accordance with your true self.
It’s very possible that the person concerned themselves doesn’t realise what’s causing their challenge. They might seek treatment just for the more visible symptoms of their condition rather than what underlies it, or another condition entirely, which is generally ineffective.
One criticism I’ve seen of the book is that it heavily focuses on a particular demographic of folk with neurodivergences - most obviously women, and in particular middle class women. There’s not a ton of discussion about the effects of poverty, race, sexuality or other intersections of identity. I can see aspects in this in terms of the suggestions of how to live a life more compatible with one’s sensitivities that are provided at times. Moving to a quieter neighborhood, redecorating your house, reading the latest research on neurodivergence or getting a new job more suited to your cognitive style are not exactly opportunities easily open to all.
Of course if you fit into this sort of demographic or know people who do, this might be a benefit rather than drawback when it comes to getting insight into yourself or others, And to be fair, many of the suggestions are more widely applicable.
The critical message of the importance of learning to accept yourself as you are and then working to accept others as they are is clearly a message that can benefit us all. If this book helps people that struggle through life for one reason or another understand they’re not alone and certainly not broken or deficient then it’ll obviously be a force for good.
On the gender front, a man with such a condition might be a little surprised at its female focus given the title doesn’t make that so clear. But I guess it acts as a counterbalance against the dominance of maleness in past psychological and medical research, a topic the book goes into some detail about when it reviews the history of psychology as a discipline. Given some of these conditions may present differently in women than men one might need to read another book on top of this one for a full understanding.
There’s also a inevitable tension here between the idea of celebrating neurodiversity versus the pathologisation of it. Under the former mindset, no-one’s thinking or sensory style is right or wrong. There’s tremendous amount of variation such that the concept of “normal” is itself largely flawed. Whether a mental tendency makes your life harder or easier is often really a product of societal and environmental choices rather than something inherent to the condition - consider the “social model” of disability. Even what we regard as a disorder certainly has changed and will again change dramatically over time.
The DSM is more like a catalogue of current social ailments than scientific hardwired “diseases.
On the other hand people do often end up as being labelled as having a disorder. Some who suffer may seek this out. This risks marking them as “aberrant”, “weird” or “sick”. Expectations may be lowered, judgements may be received. But such a label unfortunately is often necessary to gain access to healthcare or support systems.
Although there can be upsides in carefully-used labels. Many people feel far better once they’ve found a label that seems to describe how they exist in the world, that what they experience is both “real” and acknowledged. It helps them understand why some parts of life feel particularly challenging whilst they may be highly proficient in others. It also makes it easier to find a support community of people like oneself. The book contains many stories of women who couldn’t understand why life seemed to be so much harder for them than others for years until finally, later in life they received a diagnosis. They often felt validated, and gained access to a language that allowed them to discuss their needs with others.
And it’s certainly hard to argue with some of the overall takeaways. Sentiments like the quote below are universally useful to bear in mind, even if it’s not something I’d say is especially particular to the issue of neurodivergence.
There’s really nothing right or wrong about people; we’re all just people doing our best…It’s important that we see differences, that we don’t deny them; but let it stop there and respond to everyone with kindness and help.
But it might well be that the often invisible, misunderstood and hard-to-classify neurodivergences are an aspect of humanity that we’re particularly bad at considering in this context. We should certainly do our best to fix that. Educating ourselves and others such that such variations in experience exist is surely an important first step in building a world that more people feel comfortable existing within.
My more detailed notes are here.
The Partygate report is here
New Boris Johnson report just dropped.
Yes, it’s the Partygate findings from the House of Commons Committee of Privileges. As expected it’s fairly damning.
A few snippets from the summary of the full 107 page report.
Our democracy depends on MPs being able to trust that what Ministers tell them in the House of Commons is the truth.
…
We established that Mr Johnson:
a) had knowledge of the Covid Rules and Guidance
b) had knowledge of breaches of the Rules and Guidance that occurred in No. 10.
c) misled the House
…
d) was deliberately disingenuous when he tried to reinterpret his statements to the House to avoid their plain meaning and reframe the clear impression that he intended to give
…
if Mr Johnson were still a Member he should be suspended from the service of the House for 90 days for repeated contempts and for seeking to undermine the parliamentary process, by:
a) Deliberately misleading the House
b) Deliberately misleading the Committee
c) Breaching confidence
d) Impugning the Committee and thereby undermining the democratic process of the House
e) Being complicit in the campaign of abuse and attempted intimidation of the Committee.
The UK is once again experiencing a heatwave, a situation likely to become ever more common whilst we fail to solve climate change. Although the temperature is not yet the giddy heights of last year’s record-setting monstrosity, which made me curious as to what exactly constitutes a “heatwave”.
It turns out it depends on where in the UK you live. One declares a heatwave when a location experiences daily maximum temperatures of at least a certain threshold for at least 3 consecutive days. But what the threshold is varies based on which county you are in, as the Met Office shows in the below map.

Boris Johnson has stepped down as a Tory MP after claiming he was “forced out of Parliament” over Partygate.
Boris Johnson and his number one supporter Nadine Dorries resigned at the end of last week. Not the usual “resigned from being a minister but still have my job as a member of parliament” type resignation, Johnson having already been forced to do that some time ago. But rather a full resignation from being a member of Parliament, including an astonishingly self-pitying and paranoid sounding statement by the former.
The next day, another Johnson loyalist, Nigel Adams, also quit, opening up the door to 3 by-elections
It’s sort of odd that having too many illegal parties ended up being the reason that Johnson felt compelled to go. But also I won’t look a gift horse in the mouth.
The bronze elephants of Spitalfields
I spotted a herd of elephants around Spitalfields, London, this weekend.

It turns out they’re a part of the Herd of Hope, which as been migrating around London over recent years. There’s an adult mother elephant and a twenty orphaned ele-kids.

Each youngster represents a real-world herd of elephants that the Sheldrick Wildlife Trust has helped survive in a world where other groups of humans are working against the ability of elephants to thrive.

Their website lists 8 challenges that us often-thoughtless humans create for the ever-decreasing number of elephants that have so far survived amongst other endangered species.
Sometimes this is as direct as killing these animals for their tusks . Poaching is the leading threat to elephants, and for that matter all endangered large mammals. But other times we’re talking about hazards further down the causal chain such as the impact of what we’re doing to the climate on the elephants' food, water and natural habitat.

TIL: Last year scientists discovered a bacteria of such relatively huge size that it’s easily visible to the naked human eye.
First found in the swamps of Guadeloupe, Thiomargarita magnifica is around 1cm in length, which is over 5000 times larger than the average microbe. It’s apparently above the theoretical limit of how large we thought bacteria should be able to grow.
When compared to most bacteria, it would be like a human encountering another human as tall as Mount Everest.
Here’s a photo via the Guardian, which describes them as the size of human eyelashes.

A further 7 federal charges have been laid against Trump, some related to his having illegally secreted classified documents around one of his homes, causing him to fall foul of the Espionage Act.
Authorities recovered highly classified materials - some so sensitive that the government officials involved in the search lacked the security clearance to review them.
All in all, I think that’s 41 indictments against Trump in recent times so far.
Learned that the built-in fc command is a quick way to check if 2 files have the same contents using the Windows command line.
fc file_1.txt file_2.txt
It’ll show the differences if there are any. Many parameters are available around what and how to compare them; type fc /? to see what they are.
Apparently it’s been there since at least 1984. I learned about it…today.
Leutner et al. provide evidence of a link between having obesity and later developing a diagnosed mental health condition.
Receiving a diagnosis of obesity significantly increased the odds for a large spectrum of psychiatric disorders across all age groups, including depression, psychosis-spectrum, anxiety, eating and personality disorders.
Whilst there’s evidence elsewhere towards the direction of causation between obesity and mental illness potentially running both ways, in this case the diagnosis of obesity usually came first.
There are many theories as to why this connection might exist presented, ranging from biological explanations such as inflammation or gut bacteria, through to more psychosocial factors, including the impact of obesity on one’s quality of life.
It also affects different demographics differently, with the risk of being later diagnosed with a mental health condition being higher in younger people and females (even beyond the usual differential in mental health diagnosis rates).
In any case we might add enhanced mental health support as a requirement for supporting people living with obesity.
On another AI note, Google is going to introduce adverts to its generative AI search/chat feature. Whilst inevitable, perhaps it won’t be long until we’re looking back fondly at that brief moment of time where we could amuse ourselves chatting to the AI-gods without being asked to buy a mattress. Let the enshittification begin.
Here’s a screenshot from Ad Age:

They’re also offering tools to allow people to make ads via the same kind of technology. This doesn’t seem entirely without risk given the present limitations of these models.
From Search Engine Land:
Advertisers can submit creative content such as images, videos, and text related to a campaign, and the AI will “remix” these materials to generate ads that target specific audiences and meet objectives like sales targets, according to the presentation.
However, there are concerns that the tool could disseminate misinformation, as AI-generated text can confidently assert falsehoods. One individual familiar with the presentation commented that the AI is optimized for converting new customers and does not have an understanding of truth.
Noticed a couple of newish ChatGPT features. Firstly there’s an official iOS app, available for free. An Android one is in the works.
Also you can now share your AI conversations via sending a link. Anyone who knows the link can open it so be careful what you include - although by default it’s at least somewhat anonymous. Personally I wouldn’t particularly trust the system with any sensitive info in the first place.
Once the recipient opens it they can read the convo and keep on chatting to the robot mastermind in a copy of the same session. It’s a snapshot though, if you continue the conversation after generating the link, the recipient doesn’t see the new bits. Official info here.

I guess the real question is for those folk who have chatGPT perform a sizeable amount of their job for them. Will they communicate with their colleagues exclusively via chatGPT links, or does that give the game away too much?
🎙 Listened to Tech Won’t Save Us podcast.

I came to it for an antidote to the recent AI mega-hype, to which it did provide some counter-balancing relief with episodes featuring experts such as Emily M. Bender of “Stochastic Parrot” fame . But the weekly show covers subjects far beyond AI.
Mashable sums it up well as :
…a healthy counter dose to the nauseating tech utopia idealism that typically surrounds Silicon Valley and its enthusiast press coverage.
It has a decent dose of philosophy in between discussions of the technology itself. The most recent episode had an interesting history of consumerism throughout the ages, leading up to the current algorithmically-spewed mess that is the results you get when you search for most categories of products via Google or Amazon.
“Consumerism is an anti-solidary machine” was one of my favourite soundbites from that one, which also hints at the show’s somewhat socialist leanings.
📺 Watched season 8 of Brooklyn 99.
Released in 2021, the final season of the surprisingly funny police comedy dropped right into a period where humanity had once again been forced to confront the horrors of police brutality after witnessing the murder of George Floyd amongst other horrific incidents. Of course a pandemic had also been raging for a couple of years.
So it had a lot to deal with in order to seem anything other than entirely silly and tasteless. Given the context, the writers did feel the need to throw away the scripts they’d already written for the first few episodes and start again. But with their new efforts I think they did reasonably well all things considered.
The pandemic references did seem to fade out after the first few episodes. But in between the various slapstick comedy japes there were obvious attempts to acknowledge and address some of the issues around bad policing and the reactions to it, cringe and otherwise. It might not be enough for anyone who just can’t see anything about policing as funny or entertaining any more, but it could have been a lot worse.
And so many fairly funny in-jokes. I wouldn’t start with this season if you’ve never seen it before. But then again what wild kind of person would ever start a show on anything other than series 1?
Cannabis is now legal for recreational use in 22 US states
A couple of months ago Delaware became the 22nd US state to legalise recreational use of cannabis. It’ll be taxed at 15% with half the revenue going to a Justice Reinvestment Fund, which is there to “improve quality of life for communities most impacted by the prohibition of marijuana and ‘war on drugs’ era policies.”
Medical usage is now legal in 38 US states in addition to Washington DC.
Here’s a map showing where and where not, courtesy of Business Insider.

In Washington state, legislation is going through the system that helps ensure its new status is respected in a practical as well as legal sense. It will be illegal to discriminate amongst job applicants based on their use of cannabis, so no mandatory pre-interview drug test and the like.
This makes sense because 1) cannabis is legal and the average employer has no business caring about what you do in your spare time when it doesn’t affect your work performance, and 2) current tests for cannabis look for the presence of it in bodily fluids rather than whether you’re “intoxicated” from it right now. You can test positive days or potentially weeks after you actually ingested the cannabis. So if the concern is around something like turning up to work high then the tests won’t help in any case.
There’ll remain some exemptions to the anti-discrimination law for certain jobs in industries like airlines or those requiring security clearance. And employers can still test you after you’re hired.
These exemptions are controversial in some quarters, with a representative from The Cannabis Alliance drawing the parallel that:
If the same approach were applied to alcohol, employers would refuse employment to anyone who enjoyed a beer or glass of wine on the weekend
Meanwhile, over here in the UK, there’s been no substantive move in legislation for years for the general use-case. At least not in a sensible direction. Cannabis remains a wholly illegal class B drug, in the same category as for instance amphetamines, whereby mere possession could in theory result in a prison sentence of 5 years and an unlimited fine. It was actually reclassified from a lesser-penalised class C drug to a class B drug in 2009, which has been its status for the vast majority of time since the 1971 Misuse of Drugs Act came into force.
There was one positive and humane move in 2018 when cannabis and some of its derivates were legalised for UK medical use. At least in theory, but seemingly it’s under such restrictive controls that it’s hardly available in practice.
The NHS details the medical conditions it’d be considered for as:
Very few people in England are likely to get a prescription for medical cannabis. Currently, it is only likely to be prescribed for the following conditions:
- children and adults with rare, severe forms of epilepsy
- adults with vomiting or nausea caused by chemotherapy
- people with muscle stiffness and spasms caused by multiple sclerosis (MS)
It would only be considered when other treatments were not suitable or had not helped.
But even when these conditions are met, patients report that the NHS rarely delivers the goods. From the BBC:
The NHS has repeatedly refused to fund medical cannabis for children with severe epilepsy, families have said.
Three prescriptions are thought to have been written for “whole plant cannabis” oil since it was legalised two years ago, campaign group End Our Pain say.
This leaves families of patients for which these medicines truly do seem to help needing to raise vast sums of money and/or access the uncontrolled black market at the risk of their own liberty in order to get hold of what they need to live a reasonable quality of life.
Chanced upon a panel from another infinitely evergreen marvel published by The Nib, RIP once again.

It’s part of Kasia Babis' Famous Moments in History, Reimagined By Centrists.
Rclone looks to be a super useful utility for anyone who works a lot with cloud storage providers. It connects to a huge number of cloud services - Google Drive, Onedrive, Dropbox, Amazon S3 and many many others, as well as more classic file transfer methods such as FTP. And then you can manage all your cloud files without caring what or where they are.
For example you can easily back up your files to a cloud service, copy files between cloud services or even mount a cloud service as a normal disk drive and use it similarly to how you use your local disk. Imagine never having to use various cumbersome web interfaces and/or install each service’s drive syncing software again.
It’s free, open source and works on Windows, Linux and Mac so almost everyone with a computer can give it a whirl.
It’s primarily a command line tool based on various Unix commands, but don’t let that put you off. There is an experimental browser interface you could try. But really the power of it makes it probably worth figuring out if you regularly have the sort of tasks to do that it might help with.
